PELVIS - ACETABULUM (HIP BONE) TUMORS AND HEMIPELVECTOMY
- Hits: 639
The pelvis is a ring-shaped flat bone with a unique anatomy, often referred to as the hip bone, composed of the iliac wing, acetabulum, and pubic rami.
Due to its anatomical location, it serves as a connection between the spine and the thigh bone (femur). Additionally, it functions to protect certain internal organs (bladder, rectum, uterus, prostate, etc.) by housing them within.

The pelvis is an anatomical region where both benign and malignant bone tumors frequently settle. The pelvis and acetabulum are among the locations where bone sarcomas and metastases are most commonly seen. All benign bone cysts and tumors can be located in the pelvic region, and their surgical treatments are similar to those in the extremities (arms and legs).
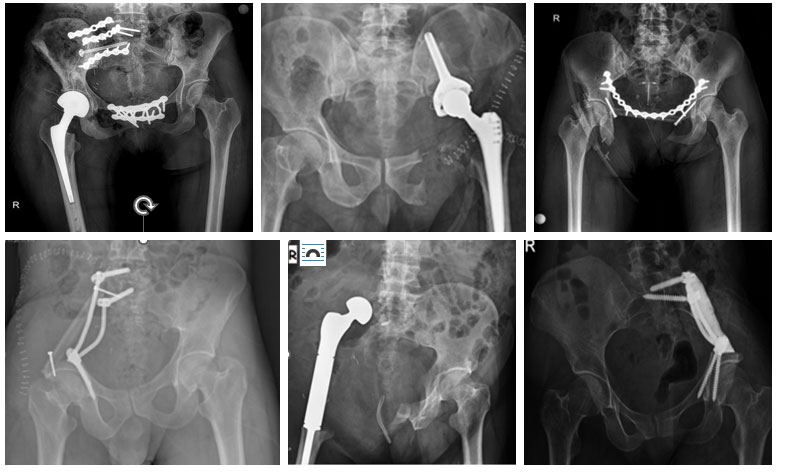
All types of cancer can metastasize to the pelvis and acetabulum region, and they metastasize to this region most frequently after the spine. The surgical treatment for many bone metastases located in the pelvis and acetabulum involves filling the void formed after cleaning the tumor (curettage) with bone cement and, in patients who require it, treating it by strengthening with fixation (plate and screw). In cases where this method is thought to be unsuccessful or insufficient, we perform resection (hemipelvectomy) and, in suitable patients, reconstruction (restructuring).
The surgical treatment of bone sarcomas (Osteosarcoma, Ewing sarcoma, and Chondrosarcoma) located in the pelvis and acetabulum is the removal (resection) of the tumor with clean, that is, wide margins. Due to the anatomical location, this surgical procedure is called hemipelvectomy. Hemipelvectomy is the highest level and most complex surgery of orthopedic oncology, requiring serious experience and meticulous planning.
Hemipelvectomy is mainly of two types: internal and external. In internal hemipelvectomy, the leg on the same side is preserved, whereas in external hemipelvectomy, the tumor is removed together with the leg.
We frequently perform internal hemipelvectomy in sarcoma cases located in the pelvis and acetabulum. However, external hemipelvectomy may be applied in recurrent cases, in cases where 2 of the 3 main structures (hip joint, sciatic and femoral nerves) cannot be preserved, in situations where major vessels (external iliac and femoral arteries) cannot be preserved and reconstructed, where soft tissue coverage cannot be provided, and in the presence of uncontrollable infection.
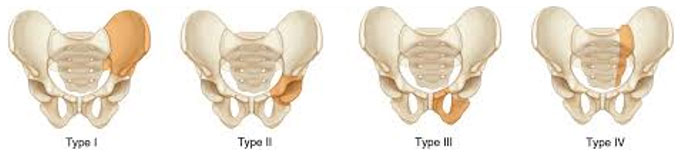
Internal hemipelvectomy is usually the removal of one entire half of the tumorous pelvic bone or a region of it, and it is typed according to the removed region. There are mainly 4 types.
Type 1: Iliac wing resection. It is a relatively easier and lower-risk resection. The formed void is often reconstructed with rods and screws and/or fibula, bone cement, recycling, and fixation. Leaving it empty after reconstruction is also an option, though we very rarely apply this method.
Type 2: Acetabulum, that is, hip joint resection. It is a relatively more complex resection type that can leave a disability. The risk of injury to the main vessels (external iliac artery and vein) and nerves (sciatic and femoral) is higher. The void formed after resection is frequently reconstructed with a prosthesis (ice-cream, LUMiC, etc.). A hip prosthesis combined with recycling is another option. Depending on the size of the tumor, resection combined with Type 1 and/or 3 can be applied.
Type 3: Resection of the pubic rami. It is a specialized surgery due to the proximity of internal organs (bladder, urethra, etc.) and major vessels (femoral artery, vein), and due to muscles (hamstring, adductor, etc.) and ligaments (sacrotuberous). The void formed after surgery is often closed with a prolene mesh to prevent hernia development. In bilateral resections, reconstruction with fibula and plate can be applied.
Type 4: Named when the sacrum is included. It is often performed together with Type 1 resection and is called sacroiliac resection. If the resection margin has to be applied closer to the inner side, injury to the nerves we call sacral roots and, although rare, consequent adverse effects on urinary, fecal, and sexual functions may develop.
In some cases, we have to combine these resections. For example, Type I+II, I+IV, Type II+III.
Reconstruction (restructuring) of the void formed after internal hemipelvectomy can be done with many different methods. Although the most frequently performed reconstruction methods are tumor prosthesis (hip transposition, ice-cream/LUMiC prosthesis, etc.), fibula, and/or recycling (liquid nitrogen or radiotherapy), leaving it empty without reconstruction can also be applied as an option. The type of resection applied, the remaining bone stock, and the general condition of the patient are particularly important in deciding on the reconstruction to be performed.
In-bed exercises are started immediately after surgery, and the patient is walked with crutches within a few days. How much weight they will put on their foot may vary according to the reconstruction technique to be performed, and walking with full weight-bearing may take a few months. Since not only the bone but also the muscles and ligaments attached to the bone are removed in these surgeries, some amount of limping may be permanent despite the best reconstruction.
Depending on the localization and size of the tumor, physicians from other branches (general surgery, cardiovascular surgery, plastic and reconstructive surgery) may need to accompany the surgery. It is recommended that such major surgery be performed in hospitals with experienced and well-equipped wards, operating rooms, and intensive care units. It is vitally important that the anesthesia team is particularly experienced. Since serious bleeding can occur in these surgeries, the anesthesia team is expected to make all preparations, including sufficient blood, and manage the process with hypotensive anesthesia.
The main risks of bone sarcoma surgeries are wound problems (infection, wound dehiscence, and gangrene/necrosis, etc.), tumor recurrence, vessel and nerve injury, serious blood loss, limitation of movement, and leg length discrepancy, especially in young children. (You can read the relevant detailed article on our website). Unfortunately, these risks (especially recurrence and wound problems) are higher in sarcoma patients with pelvis and acetabulum localization. Due to the presence of a large surgical wound, the surgery taking hours, a void remaining inside after the tumor is removed (even if reconstruction is performed, due to the removed muscles), the risk of wound problems (infection, wound dehiscence, and necrosis, i.e., gangrene at the wound edges) is high. Due to wound problems, patients may require long hospital stays, recurrent wound debridement, VAC applications, and even soft tissue reconstructions (flap surgery). In addition to these risks, internal organ (bladder, bowel, etc.) injuries and incisional hernias may also develop. Ultimately, life-threatening risk is unfortunately a reality for these surgeries, albeit very rarely. Serious experience, meticulous planning, and close follow-up are required to reduce these risks as much as possible.