SACRAL TUMORS AND SACRECTOMY
- Hits: 594
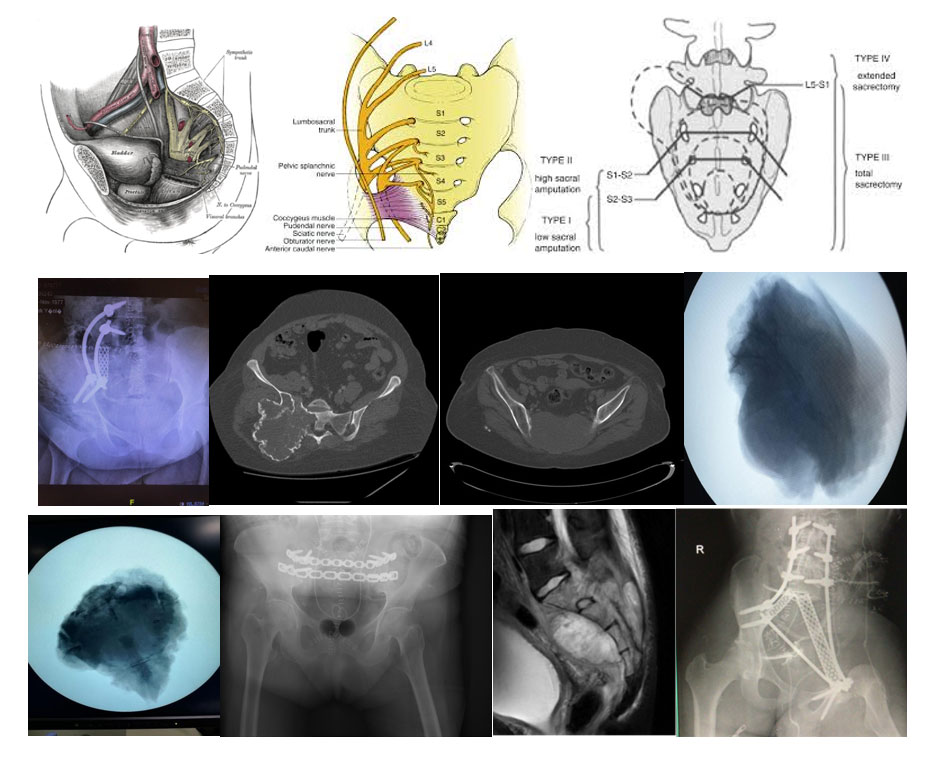
The sacrum is a special bone composed of five distinct bones (S1-5) with a unique anatomical structure that provides the connection between the spine and the pelvis, housing the sacral nerve roots (S1-4).
Among the sacral roots contained within it, the S1 root is responsible for the sensation of the sole of the foot and the function of pressing the foot downwards (plantar flexion). The S2-4 nerve roots (pudendal nerve) are responsible for the sensation of the perineal region, as well as urinary (bladder, urethra), fecal (rectum, anus), and sexual functions. In tumors located in the sacrum, a loss in these nerve functions may be observed due to either the tumor itself or damage that may occur during surgery. Depending on the location and extent of the damage, these may develop as loss of sensation and movement in the foot, urinary and fecal incontinence or retention, and sexual dysfunctions (erectile dysfunction, etc.).

Since the sacrum serves as a load transfer point between the spine and the pelvis due to its location, difficulty in sitting and walking may develop due to bone destruction caused by the tumor or the surgery. We overcome this adverse situation by placing titanium implants, which we call screws and rods, between the spine and the pelvis (Lumbopelvic fixation).
The sacrum is an anatomical location where both benign and malignant bone tumors settle.
BENIGN BONE TUMORS LOCATED IN THE SACRUM
Many benign bone tumors (simple bone cyst, aneurysmal bone cyst, osteoblastoma, fibrous dysplasia, etc.) can be located in the sacrum; however, since it is one of the typical locations for giant cell tumors, we will provide more detailed information about this in this article. Detailed information about other benign bone tumors can be found in the relevant articles on our website.
Giant Cell Tumor of Bone
The cause and the tissue of origin are not exactly known. The sacrum is one of the typical locations in the spine. The giant cell tumor of bone is a tumor we call locally aggressive, which causes destruction in the bone where it is located and is prone to recurrence (relapse) after surgery. Patients usually apply to the physician with pain and swelling; however, in sacral locations, signs of nerve damage (numbness, tingling, weakness, urinary, fecal, and sexual dysfunctions) may develop. Since the complaints are not very typical, they may exist for a long time and can be confused with other diagnoses (lumbar disc herniation, sacroiliitis, etc.). Patients usually state that their complaints increase over time.
Due to the location of the sacral giant cell tumor (bowel gas shadows), it may not give findings on direct radiography (X-ray) and can be missed. The location, boundaries, and extent of bone damage of the tumor are revealed in detail by Tomography (CT), while the soft tissue component outside the bone and nerve roots are revealed by contrast-enhanced MRI. In giant cell tumors of bone, the diagnosis is confirmed by a biopsy procedure performed after clinical and radiological evaluation. The biopsy procedure is often performed as a closed procedure under local anesthesia, accompanied by imaging (fluoroscopy or tomography) with the help of special needles (Jamshidi). It is important that the orthopedic surgeon performing the biopsy and the pathologist examining the samples are experienced in the field of bone and soft tissue tumors.
Although the giant cell tumor of bone is benign, unfortunately, it can metastasize to the lung, albeit very rarely (3-5%). Therefore, a patient with a confirmed diagnosis should primarily be screened for lung metastasis (Thorax CT). The main treatment for giant cell tumor of bone is the surgical removal of the tumor. For this, the tumor is scraped out of the bone using a method we call curettage. To reduce the possibility of recurrence, we routinely apply aggressive curettage with adjuvant methods (cautery, burr, phenol, alcohol, hydrogen peroxide, liquid nitrogen, etc.), but we can only perform this procedure to a limited extent in the sacrum due to the proximity of nerve roots. Therefore, the probability of recurrence in tumors located in the sacrum is unfortunately higher than in those located in the extremities (arms, legs). The void formed after the removal of the tumor is often filled with bone cement.
In patients who develop bone weakness (insufficient stability) caused by the tumor or surgery, we can perform strengthening (fixation) processes with different methods. Additionally, since tumors in this region are more prone to bleeding, preoperative embolization (blocking the vessel feeding the tumor via angiography) is recommended. Denosumab is a type of bone-strengthening drug used in giant cell bone tumors. In sacral giant cell tumors, we may resort to denosumab treatment, especially in cases where bone destruction is advanced, surgery is very risky and cannot be performed, and in recurrent cases. How long denosumab treatment should be used is controversial and should be decided according to the patient. There is a risk of tumor recurrence in patients whose denosumab treatment is stopped. Radiotherapy is another treatment method in similar situations, but both methods should be resorted to in selected cases after a very careful evaluation. Because there is a risk of transformation from benign to malignant (malignant giant cell tumor) after both methods. We rarely perform partial sacrectomy in sacral giant cell bone tumors. Treated patients should be followed closely for many years at certain intervals regarding recurrence.
MALIGNANT BONE TUMORS
These can be divided into two main groups: Primary, which originates from the bone itself, and Secondary, that is, metastasis, which originates from another organ and spreads to the bone.
1. Bone Metastases
They frequently occur in the spine and pelvis region, and the sacrum is a rare location among these sites. We primarily benefit from chemotherapy and radiotherapy in bone metastases. We resort to surgical treatment in patients who do not achieve sufficient results with both methods. We frequently perform curettage and cement application, especially in cases of tumor growth despite treatment, persistent severe pain, development of numbness, tingling, weakness, urinary, fecal, and sexual dysfunction due to nerve root compression, and development of difficulty in sitting and walking due to severe bone destruction. Our priority during surgical intervention is the protection of nerve roots and their relief from tumor compression. We frequently see insufficiency fractures (stress fractures) in the sacrum, especially due to radiotherapy. In these cases, we can obtain successful results from closed cementing (sacroplasty) application accompanied by imaging.
2. Bone Sarcomas
Other malignant bone tumors located in the sacrum are Osteosarcoma, Ewing sarcoma, and Chondrosarcoma. These tumors are generally located in the extremities (arms, legs) and pelvis. Chemotherapy is administered before and after surgery in Osteosarcoma and Ewing sarcoma. Radiotherapy can also be applied in Ewing sarcoma if needed. Since Chondrosarcoma is resistant to chemotherapy and radiotherapy, its main treatment is the surgical removal of the tumor with clean margins. We perform surgical sacrectomy in all three types of sarcomas located in the sacrum. Depending on the size and location of the tumor, total or partial sacrectomy can be performed. The goal here is to remove the tumor by performing a wide resection with clean margins. For this purpose, sacral nerve roots may be sacrificed considering the damage it will leave. You can access detailed information about sarcomas from the relevant article on our website.
Among the primary malignant tumors located in the sacrum, we encounter Chordoma most frequently. Therefore, we will give more detailed space to this subject in this article.
3. Chordoma
It is a slow-progressing bone cancer (a long time may pass from its emergence to the moment of diagnosis) originating from notochord remnants. Chordoma is most frequently located in the sacrum and the neck region of the spine. Patients often apply to the physician with pain and swelling. Due to proximity, they are frequently confused with lumbar problems (herniated disc, stenosis, etc.). Since it can compress the rectum in very large tumors, constipation may develop in patients. Especially in tumors with bilateral and multi-level nerve compression, numbness, tingling, weakness in the soles of the feet, urinary and fecal control disorders, and sexual function insufficiencies may develop.
Due to its location (shadowing of bowel gases), it may not give a finding on direct radiography (X-ray) and can be missed. The location, boundaries, and extent of bone damage of the tumor are revealed in detail by Tomography, while the soft tissue component outside the bone and nerve roots are revealed by contrast-enhanced MRI. Its relationship with neighboring organs is evaluated in detail, and surgical planning is made. In giant cell bone tumors, the diagnosis is confirmed by a biopsy procedure performed after clinical and radiological evaluation. The biopsy procedure is often performed as a closed procedure under local anesthesia accompanied by imaging (fluoroscopy or tomography) with the help of special needles (Jamshidi). It is important that the orthopedic surgeon performing the biopsy and the pathologist examining the samples are experienced in the field of bone and soft tissue tumors.
Thorax tomography and vertebral magnetic resonance imaging (MRI) should be performed for metastasis screening in the diagnosed patient. Since Chordoma is resistant to chemotherapy and radiotherapy, its main treatment is the removal of the tumor with clean margins. For this purpose, total or partial sacrectomy is applied according to the location of the tumor. Carbon ion or proton therapy can be applied in cases unsuitable for surgical treatment or recurrent cases; however, these two methods are not available in our country and can be applied in certain centers abroad and are very high cost.
SACRECTOMY
Sacrectomy is the name given to the removal of the sacrum together with the tumor, applied in malignant bone tumors located in the sacrum (Chordoma, Osteosarcoma, Ewing Sarcoma, Chondrosarcoma, etc.). We can also perform sacrectomy in very large or recurrent giant cell bone tumors that very rarely cause severe bone destruction. Sacrectomy is one of the most specific and experience-requiring surgeries applied for bone tumors.
Sacrectomy can be performed mainly in two different ways: total and partial. It is also classified into 4 distinct types (Type I Low: below S2-3 level, Type II High: below S1-2 level, Type III Total: including S1, Type IV Extended: including lumbar spine). We can apply different incision methods depending on the location and size of the tumor. We frequently perform the sacrectomy surgery with the patient in a prone position, entering from above the coccyx.
Especially in total sacrectomy cases where the first sacral bone must be removed, the patient must first be opened from the front (Laparotomy) together with a general surgeon to release and protect the main vessels (aorta, iliac arteries and veins, sacral arteries and veins, etc.) and organs (especially the rectum) in front of the sacrum. Since bowel dysfunction will develop in patients undergoing total sacrectomy, a colostomy is opened simultaneously with laparotomy, and the defecation function is taken to a bag from the front of the abdomen. We primarily apply a catheter for urinary function.
To reduce blood loss in sacrectomy surgery, we can perform a procedure called embolization, which blocks the vessels feeding the tumor, especially before total sacrectomy surgery for large tumors. Specifically, in patients where we perform total sacrectomy, we perform lumbopelvic fixation with titanium screws and rods to maintain the connection between the spine and the pelvis. For this purpose, we can also apply titanium cages and fibula bone. Depending on the size and extension of the tumor, a part of the vertebra or pelvis bone may need to be removed together with the sacrum.
Apart from functional disorders due to nerve loss, the biggest risks of sacrectomy surgery are wound problems and tumor recurrence. Since the surgical wound is close to the perineal region due to its location, the risk of infection is high. Additionally, especially in malignant tumor surgeries, since some surrounding healthy muscle tissues will also be removed to remove the tumor with clean margins, we may encounter gangrene (necrosis) and dehiscence (opening) in the wound due to the void formed and nutritional problems. To minimize possible wound problems, good planning, respect for tissue during surgery, and, if necessary, entering the surgery with a reconstructive surgeon/microsurgeon to plan soft tissue coverage (flap surgery) should be done.
Due to the void formed after the tumor is removed, seroma accumulation and drainage may develop. Therefore, it may be necessary to keep the existing drains for a long time. One of the general risks of malignant bone tumor surgeries is the recurrence of the tumor. Unfortunately, this risk is higher in sacral surgeries, especially in patients diagnosed with Chordoma, due to the anatomical localization. One of the reasons for this is the difficulty in reaching wide resection margins due to neighboring vital organs. The biggest reason for this risk being higher in Chordoma patients is its resistance to chemotherapy and radiotherapy. Therefore, patients should be followed up for many years at certain intervals. Re-treatment planning is made for patients who develop recurrence.